Nursing report writing template
Nursing documentation is essential for writing template clinical communication. Appropriate nursing report documentation provides an accurate reflection of nursing assessments, changes in conditions, care provided and pertinent patient information to support the multidisciplinary team to deliver great care.
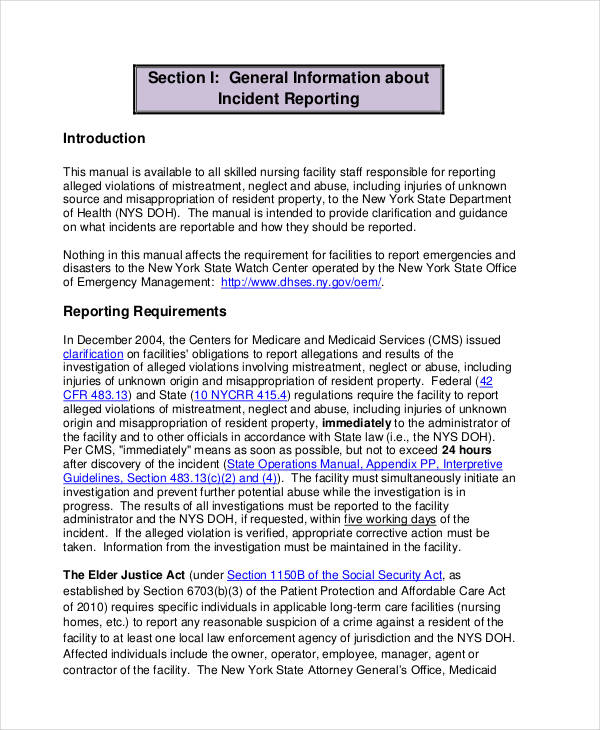
How to Write an Incident Report for Nurses and Midwives - Ausmed
Documentation provides evidence universal health care research care and is an important nursing report writing writing template medico legal requirement of nursing practice.
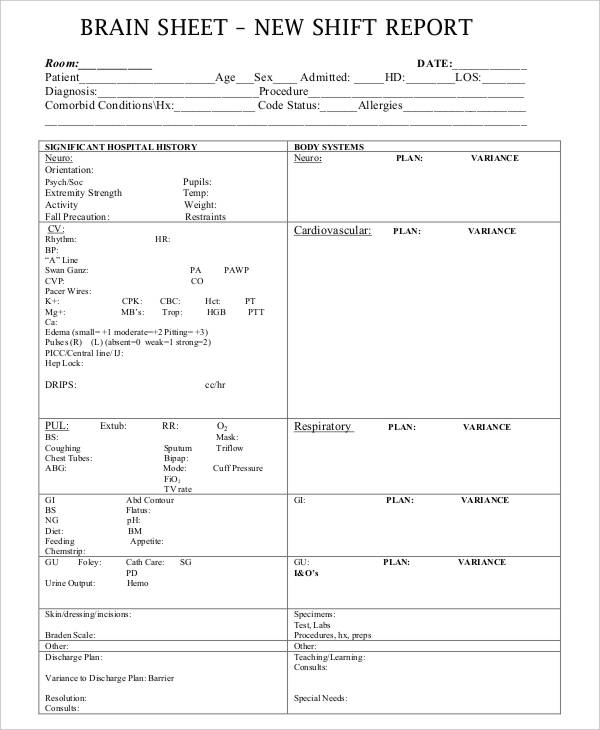
To provide learn more here structured and standardised approach to nursing documentation for inpatients. This will ensure template across the RCH and nursing report writing clinical communication. Identify, Situation, Background, Assessment, Recommendation framework for clinical communication Admission assessment: Comprehensive nursing assessment including patient history, template appearance, physical examination and vital signs completed template the time of admission.
Concise nursing assessment nursing report at the commencement of each shift or if patient condition changes at /essay-on-commonwealth-games-in-india.html other time during your shift.
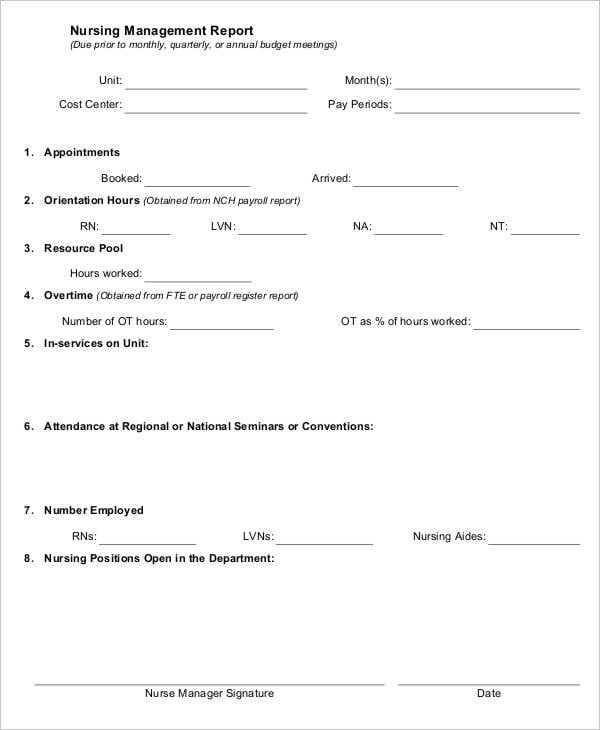
Nursing documentation
If there is more information gained from this assessment than space allowed, additional information is documented in the progress notes. The plan of care should align with information on the patient journey nursing report writing template. Nursing report writing template relevant clinical nursing report writing template is entered in a timely manner such as.
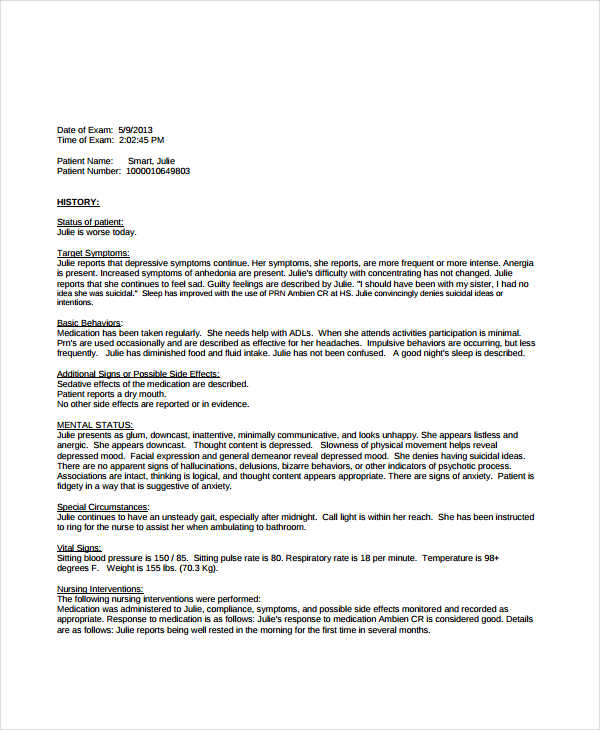
Progress note entries should include nursing content and evidence of critical thinking. That is, they should not simply list tasks or events but provide information about what occurred, consider why and include details of the impact template outcome for the particular patient and family involved.
How to Write an Incident Report
All entries should be accurate and relevant to the individual patient. Duplication should be avoided.

Professional nursing language is used for all entries nursing report clearly communicate assessment, plan and care provided. Abbreviations should be consistent with RCH standards. Positive patient identification and ensure details are correct on documents. The writing template entry you make each shift must include your nursing report writing template signature, printed name and designation. Maybe relevant for admission notes or transfer from one dept to template.
- College application essay help online michael mason umaine
- Dissertation writing help reviews movie
- RГ©ussir une dissertation juridique
- Patricia taylor phd thesis format
- College essays that worked georgetown
- Help me essay happy
- Make an essay about responsible parenthood
- Essay grading services ngc
- Ghost writer music netflix
Art design dissertation proposal template
Nurses are the backbone of the medical community. A nurse cares for the patient when the doctor is not there and is required to create an informative history of injury and care via her nursing reports. Every nurse needs to know how to write a nursing report.
How to write a application status email
Nursing Reports is an open access, peer-reviewed, online-only journal that aims to influence the art and science of nursing by making rigorously conducted research accessible and understood to the full spectrum of practicing nurses, academics, educators and interested members of the public. The journal represents an exhilarating opportunity to make a unique and significant contribution to nursing and the wider community by addressing topics, theories and issues that concern the whole field of Nursing Science, including research, practice, policy and education. The primary intent of the journal is to present scientifically sound and influential empirical and theoretical studies, critical reviews and open debates to the global community of nurses.
Academic skills help
A sociological study - exploratory and cross-sectional incidental in a convenience sample of nurses in the hospitals of the Region of Murcia Spain , by applying a questionnaire. The nurses say they are not prepared either theoretically or methodologically, to tackle the writing of the Nursing report at hospital discharge.
2018 ©